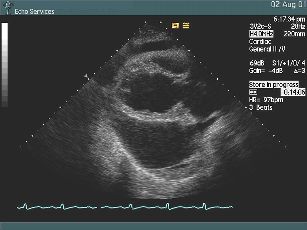
 The initial Parasternal Long Axis view gives an understanding to this patient's severe chest pains. The dark anechoic area surrounding the heart is a very large pericardial effusion. The heart swings within this space and there is right ventricle collapse during the cardiac cycle, which are signs of cardiac tamponade. The greatest effusion volume is located posteriorly to the left ventricle.
The initial Parasternal Long Axis view gives an understanding to this patient's severe chest pains. The dark anechoic area surrounding the heart is a very large pericardial effusion. The heart swings within this space and there is right ventricle collapse during the cardiac cycle, which are signs of cardiac tamponade. The greatest effusion volume is located posteriorly to the left ventricle.